
Rationale for NanoStilbene/EGCg Conjugate in Endothelial Dysfunction
Augmentation of Stem Cell Activity using Pterostilbene and Epigallocatechingallate
Discussed are means of augmenting circulating endogenous stem cells through administration of an effective amount of pterostilbene and epigallocatechingallate (EGCg). In one application a patient with reduced levels of circulating endothelial progenitor cells can be supplemented with NanoStilbene alone, at a concentration and frequency sufficient to restore, and/or enhance levels of circulating endothelial progenitor cells (EPC). In another application endogenous levels of stem cells are restored or enhanced by administration of NanoStilbene and EGCg. Cells may include endogenous stem cells comprised of the dentate gyrus, subventricular zone, hepatic stem cells, cardiac stem cells, and hematopoietic stem cells.
Pterostilbene is a phenolic compound biologically classified as a phytoalexin, which is an antimicrobial substance that is part of a plant’s defense system and is synthesized in response to pathogen infection, as well as to excessive ultraviolet exposure.
Pterostilbene is known to have diverse benefits for the prevention and treatment of wide variety of diseases, including cancer, diabetes, cardiovascular disease and cognitive function degeneration.
Accordingly, the use of pterostilbene for acceleration of healing and revascularization by augmentation of EPC numbers and/or potentiation of activity is discussed.
One of the first targets of atherosclerotic disease is the penile vasculature [1]. Accordingly, the use of pterostilbene, and analogues thereof, to augment vascular function, and through this to augment health and prevention of vascular associated diseases is reviewed.
In general, atherosclerotic disease is correlated with decreased levels of circulating EPC. One study assessed patients without cardiovascular disease having varying scores on the Framingham risk questionnaire. A correlation between higher risk scores and low EPC numbers was found [2]. Another study assessed the preclinical atherosclerosis marker of carotid intima-media thickness (IMT) measured by ultrasound. The investigators found a correlation between IMT and low levels of CD34+, KDR+ circulating EPC.
Patients with atherosclerosis have been described by numerous studies as having reduced numbers of EPC compared to healthy controls [3,4,5,6]. Additionally, correlations between stenosis and reduced circulating EPC numbers have also been made [4]. Thus, given the hypothesis that ED is caused in many cases by atherosclerotic disease, it should not be surprising that several studies have found patients with ED as having suppressed numbers of circulating EPC. Accordingly, we teach here, the use of pterostilbene alone, or in combination with other therapeutic modalities, as a treatment for erectile dysfunction.
Foresta et al reported lower number of cells capable of forming CFU-E in circulation of men with ED as compared with healthy controls. Their rationale was based on previous reports of cardiovascular disease affecting the penile circulation first, and given that cardiovascular disease correlates with lower EPC, they sought to verify if ED was an early manifestation of cardiovascular disease [7].
A subsequent study of 119 patients with coronary artery disease found that almost 60% had ED. Presence of ED correlated with known cardiovascular risk factors such as age, hypertension, reduced left ventricular ejection fraction (LVEF) and diabetes. Importantly, ED correlated with reduction in circulating EPC [8]. A similar correlation was found in a study comparing 30 healthy overweight men with 30 overweight men suffering from ED. Severity of ED according to the IIEF score correlated with lower numbers of EPC [9].
Chronic inflammation has been associated with ED and with a variety of chronic degenerative diseases. Assessment of inflammatory markers followed by modification of pterostilbene dosage after identifying to what extent modulation of inflammatory markers has occurred should be determined.
In the case of ED, a study of 137 men with ED found significant association between the levels of the inflammatory marker C-reactive protein (CRP) and severity of penile vascular disease as measured by penile Doppler [10]. In obese men, presence of ED was also associated with increased CRP-levels [11]. Oxidative stress plays a known component in numerous inflammatory conditions. In ED, salivary 8-hydroxy-2′-deoxyguanosine, a known marker of oxidative stress, has been shown to correlate with severity of dysfunction [12].
Numerous other markers of oxidative stress have been associated with ED including upregulation of the hypoxia inducible factor-1alpha (HIF-1alpha), superoxide dismutase (SOD), aldose reductase (AR) and nerve growth factor (NGF) genes [13]. Other inflammatory mediators such as TNF-alpha are associated with ED [14]. Interestingly mice lacking TNF have increased erectile ability [15], whereas administration of TNF to corpora cavernosa tissue ex vivo results in decreased reactivity [16].
Additionally, increased systemic levels of TNF are observed in a form of inflammatory arthritis called ankylosing spondylitis. Treating these patients with TNF inhibitors results in increased erectile function [17]. The detection of these types of inflammatory markers may be used to titrate the dose of NanoStilbene.
Thus, it appears that underlying chronic inflammation associated with atherosclerotic disease has a negative effect on circulating EPC, which may account for impaired endothelial repair and poor vascular function associated with ED. Supporting the inflammatory cause of EPC decrease are studies in which anti-inflammatory agents partially, or fully restore EPC numbers similar to healthy controls.
For example, Grisar et al demonstrated in 28 patients with rheumatoid arthritis that a 7-day course of treatment resulted in restoration of circulating EPC to values comparable to healthy age-matched controls [18].
Green tea has been reported to contain numerous antioxidants [19]. Given the known component of oxidative stress on inflammation, as well as the direct anti-inflammatory role of components in green tea, an investigation was conducted in 20 young smokers to determine whether green tea administration altered circulating EPC [20]. Consumption of green tea daily for 2 weeks resulted in an increase in circulating EPC, as well as improvement in endothelial function as measured by the flow mediated dilation assay (FMD).
In the specific case of ED, administration of the antioxidant vitamin alpha-tocophenol resulted in IIEF improvement in a pilot group of patients resistant to PDE5 inhibitors [21].
Other antioxidants have displayed benefit in ED including folic acid [22], Korean ginseng [23], and propionyl L-carnitine [24].
Thus, it appears that in ED a low grade, underlying inflammation, associated with markers such as CRP, TNF-alpha, as well as oxidative stress, are associated with reduction in EPC numbers and possibly causative of pathology.
The bone marrow is recognized as a major source of EPC. Suggestive of the angiogenic potential of bone marrow was an early clinical study by Tateishi-Yuyama et al, in which 22 patients with bilateral critical limb ischemia were treated intramuscularly with autologous bone marrow mononuclear cells in randomly chosen legs, with control leg receiving peripheral blood derived mononuclear cells [25]. Improvement in the treated legs was observed in terms of ankle brachial index, pain-free walking and ulcer healing. One of the primary characteristics of endothelial dysfunction is reduction in the flow mediated dilation assay. In an attempt to induce neo-angiogenesis through stimulation of circulating EPC numbers, mobilization of bone marrow progenitors was performed by 2-week administration of GM-CSF in 45 patients with peripheral arterial disease [26].
At 12 weeks not only was improvement in exercise capacity noted (as compared to pre-treatment levels), but also systemic augmentation of the flow mediated dilation assay was reported. These data suggest the possibility that administration of cells containing EPC, such as bone marrow, as well as mobilization of endogenous bone marrow EPC may be useful in repairing/improving endothelial function.
Unfortunately, autologous bone marrow therapy and mobilization by agents such as GM-CSF is cost-prohibitive and possesses possibility of undue pain to the patient. In the case of autologous bone marrow, the need to perform iliac crest extraction to collect sufficient cell numbers is difficult to perform in patients that numerous times have a variety of comorbidity conditions.
The use of cytokine-based mobilization, if used chronically, can lead to splenomegaly, bone marrow hyperplasia, and other adverse effects. The use of pterostilbene together with mobilizers of bone marrow stem cells is may be considered. In animal models, administration of agents capable of inducing endothelial cell proliferation, and/or neoangiogenesis, induces inhibition of ED progression or reversion of ED.
For example, basic fibroblast growth factor (bFGF) is a known inducer of angiogenesis in ischemic situations, and its exogenous administration is therapeutic in models of stroke [27], angina [28], and peripheral limb ischemia [29]. The administration of two 2.5 microgram doses of bFGF, at 3-week intervals into corporal tissue of hypercholesterolemic rabbits was shown to increase corporal relaxation in response to chemical stimuli, as well as ability to generate NO [30].
In another study, intracavernous administration of bFGF into diabetic rats by means of gelatin microbeads resulted in protection of erectile function [31]. Additionally, another study demonstrated that systemic basic fibroblast growth factor induces favorable histological changes in the corpus cavernosum of hypercholesterolemic rabbits [32].
The use of pterostilbene, in one manner, may also comprise of augmentation of activity of known agents that stimulate EPC numbers, said agents include: Testosterone administration to hypogonadal men increases erectile function while simultaneously stimulating numbers of circulating EPC [33]. Interventions such as exercise [34], and smoking cessation [35], which have demonstrated improvement in erectile function are also associated with augmentation of circulating EPC [36, 37, 38].
Green Tea Extracts – (trihydroxyphenolic units)
EGCG (epigallocatechin gallate) is a major polyphenol found in green tea, along with ellagic acid, epicatechin gallate, epigallocatechin, gallocatechin, epicatechin, and catechin.
The biological pathway identified here involves trihydroxy- containing polyphenols at concentrations achievable by dietary ingestion. Indeed, foods rich in this class of compounds, such as EGCG, have been consumed as therapeutics for decades [39].
A large number of clinical trials have demonstrated that tea is good for health in terms of the prevention and treatment for a range of diseases, such as cardiovascular disease [40], lung cancer [41], breast cancer [42], prostate cancer [43] and pathogenic microorganisms, etc. For example, tea consumption may be able to interrupt the chronic progress of atherosclerosis and thus prevent or delay the onset of ischemic stroke. Tea may also protect the artery wall by reducing blood pressure, inhibiting the migration of monocytes and smooth muscle cells to the atherosclerotic lesion, inhibiting proliferation of smooth muscles cells, and by improving endothelial function [44].
One cup of tea provides 150-300 mg flavonoids [45]. The mounting evidence that tea flavonoids can improve endothelial function and lower blood pressure has emerged in recent years. A report in 2006 showed that short-term administration of green tea in 20 young healthy smokers induced a rapid improvement of endothelial progenitor cell levels and flow-mediated endothelium dependent vasodilation.
Green tea consumption may be effective in preventing future cardiovascular events in chronic smokers [46]. A Japanese study found that green tea consumption over short and long periods appeared to ameliorate endothelial dysfunction by scavenging free radicals with anti-inflammatory and anti-apoptotic properties in healthy male smokers [47].
Endothelial dysfunction has been associated with coronary artery disease and increased oxidative stress. Duffy et al [48] randomized 66 patients with proven coronary artery disease to consume black tea and water in a crossover design; they found that short- and long-term black tea consumption reverses endothelial vasomotor dysfunction in patients with coronary artery disease. Some antioxidants have been shown to reverse endothelial dysfunction and tea contains antioxidant flavonoids.
A proposed mechanism by which dietary flavonoids could affect flow-mediated endothelium dependent vasodilation is that they improve the bioactivity of the endothelium derived vasodilator nitric oxide (NO) [49] by enhancing NO synthesis or by decreasing superoxide-mediated NO breakdown. Flavonoids may increase endothelial NO production by stimulating Akt-mediated endothelial-derived NO synthase activity and additionally decrease levels of the vasoconstrictor endothelin-1[50,51].
A study recently reported the vasoconstrictor actions of exogenous endothelin-1 and methoxamine to be mediated by the RhoA/Rho-kinase pathway in the cavernosal circulation. While it is widely recognized that the nitric oxide-cyclic GMP-protein kinase G pathway mediates vasorelaxation and penile erection, the interaction between this pathway and the vasoconstrictor process remains to be fully elucidated. During erection, the vasoconstrictor action of methoxamine and endothelin -1 are inhibited and NO is likely to be responsible for this inhibition [52].
Erectile dysfunction in men over 40 years of age is usually of vascular (endothelial dysfunction) origin [53].
In other words, endothelial dysfunction is a causative factor in the development of erectile dysfunction. As flavonoids of tea may decrease erectile dysfunction occurrence as it may ameliorate endothelial dysfunction, we therefore hypothesize that the conjugate of NanoStilbene and our proprietary Green Tea Extract may play a role in erectile dysfunction prevention.
NanoStilbene
Pterostilbene, being extracted from many plants, has significant biological activities in preventing cancer, diabetes, and cardiovascular diseases so as to have great potential applications in pharmaceutical fields. But the poor solubility and stability of pterostilbene strictly restrained its applications. As a good protection and oral delivery system, an optimal nanoemulsion for pterostilbene was developed by using a low-energy emulsification method.
Nanoemulsions are non-equilibrium systems and possess kinetic stability in a long period with a remarkable small droplet size (below 200 nm).
The pterostilbene placed in a nanoemulsion droplet is free from air, light, and hard environment; therefore, as a delivery system, nanoemulsion can not only improve the bioavailability of pterostilbene but also protect it from oxidation and hydrolysis, while it possesses an ability of sustained release at the same time.
The “NanoStilbene” is prepared by method of low-energy emulsification which includes a phase inversion composition (PIC). The low-energy emulsifying method possesses great advantages of lesser physical destruction of active agents, smaller size of droplets, better phase behavior, and more convenient industrial scale-up than high-energy emulsifying methods.
In the PIC process, the stability and droplet size are greatly influenced by oil/surfactant ratio, hydrophile-lipophile balance (HLB) of surfactants.
We therefore aimed at developing an optimal oil/water (O/W) pterostilbene nanoemulsion by the PIC method on the basis of minimum surfactant concentration with increases in the solubility, stability, and the release performance of pterostilbene.
Nanotechnology
Therapeutic uses of nanotechnology typically involve the delivery of small-molecule drugs, peptides, proteins, and nucleic acids. Nanoparticles have advanced pharmacological effects compared with the therapeutic entities they contain. Active intracellular delivery and improved pharmacokinetics and pharmacodynamics of drug nanoparticles depend on various factors, including their size and surface properties.
Nanoparticle therapeutics is an emerging treatment modality in cancer and other inflammatory disorders. The National Cancer Institute has recognized nanotechnology as an emerging field with the potential to revolutionize modern medicine for detection, treatment, and prevention of cancer.
On May 15, 2018 TSI announced Institutional Review Board (IRB) clearance to initiate a pilot pharmacokinetic trial of “NanoStilbeneÔ.” Then on July 02, 2018 the Company announced receiving pilot clinical data providing proof of concept that NanoStilbene more effectively increases blood levels of the molecule as compared to conventional formulations. The clinical trial involved the administration of NanoStilbene in comparison to powder in capsule form pterostilbene with healthy volunteers, whom underwent a series of blood draws to determine the concentration of the compound.
Blood was collected in EDTA tubes and plasma collected subsequent to centrifugation at 700g for 10 minutes. Collection time points were prior to administration of test compound, as well as at times 2hr, 4hr, 6hr, 8hr, 10hr, and 12 hrs. Test compounds were 10 ml of NanoStilbene (provided by Therapeutic Solutions International) and 6 capsules of 50 mg pterostilbene (
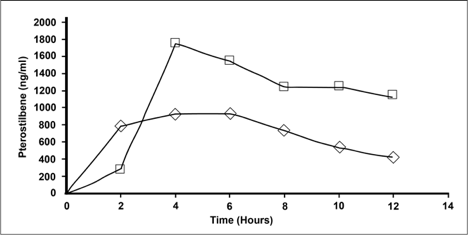
The results were that at peak concentration NanoStilbene (Square) had a 55% increase in serum levels over the traditional powder (Triangle) form of pterostilbene. The data also shows the half-life to be double to that of the powder form.
The data in Granted U.S. Patent No.: 9,682,047 strongly suggest that pterostilbene administration may be an inexpensive and safe method of augmenting the efficacy of numerous immunotherapeutic drugs. Although cancer immunotherapy has revolutionized the prognosis of many patients, the majority of patients still possess poor or suboptimal responses to this approach.
Quantification of Pterostilbene
Plasma levels of pterostilbene was measured using a tandem mass spectrometer (API 3000; Applied Biosystems/MDS Sciex, Foster City, CA) equipped with a high performance liquid chromatograph (Agilent 1200; Agilent Technologies, Wilmington, DE). For pterostilbene determination, a 100 μL aliquot of plasma was mixed with 1 mL of acetonitrile (ACN; Sigma–Aldrich, St. Louis, MO). After vortex mixing for 1 min, the sample was centrifuged at 7,000 RPM at 4°C for 10 min to remove precipitated proteins; the supernatant was transferred to a clean tube and dried under nitrogen at room temperature (approximately 25°C). After the evaporation was completed, the residue was reconstituted in 100 μL of methanol with 5 min of sonication, added to 400 μL of water, vortex mixed, and centrifuged again. The resulting supernatant was transferred to a sample vial for instrumental analysis. All sample preparations were conducted under yellow light and using opaque plastic ware to avoid light exposure of the agent.
Freshly prepared pterostilbene standard curves were analyzed along with samples on each day of analysis. Instrument calibrators and quality control (QC) samples were prepared by adding 10 μL of a stock pterostilbene solution (in a methanol/water mixture [v/v 50:50] to 100 μL of rat plasma (Bioreclamation Inc., Westbury, NY). Target calibrator concentrations were 5, 10, 20, 50, 100, 200, 500, and 1,000 ng/mL. QC samples were prepared at approximately 12, 400, and 800 ng/mL. Calibrators and QC samples were processed for analysis using the procedure described earlier. The concentration of conjugated metabolites for both agents was estimated using the calibration curve for each parent compound.
Chromatography was performed using a Luna 3μC18, 30 × 2.0 mm column (Phenomenex, Torrance, CA) maintained at a temperature of 25°C. A flow rate of 0.25 mL/min was used. Mobile phase (MP) A consisted of 5 mM ammonium acetate in water:isopropanol (98:2, v/v); and MP B consisted of methanol:isopropanol (98:2, v/v). The MP gradient was as follows: after injection, initial conditions with MP A at 90% were held for 0.5 min, decreased to 5% in 3.5 min and held constant for 5 min, returning to initial conditions for another 3 min of re-equilibration time. Retention times for the target analytes were: pterostilbene, 6.3 min; pterostilbene glucuronide, 5.4 min; and pterostilbene sulfate, 5.5 min. Total run time was 12 min.
A turbo ion spray interface was used as the ion source operating in negative ion mode. Acquisition was performed in multiple reaction monitoring mode using the following ions: pterostilbene, 255.1 → 197.5; pterostilbene glucuronide, 431.1 → 255.1; and pterostilbene sulfate, 335.1 → 255.1. Ion spray voltage was −3,000 V; ion source temperature was 450°C; and collision energy was −30, −35, or 45 V.
The selectivity of the method was assessed by analyzing plasma extracts from different lots for the presence of analytical interferences and comparing the results to those obtained from spiking the blank plasma sources with analytes at the lower limit of quantitation (LLOQ; 5 ng/mL). Linearity was assessed using external standard method (pterostilbene) and up to eight calibrators with analyte concentrations in the 5–1,000 ng/mL range. The curves were built from peak areas using least-squares linear regression with (1/x) weighting factor. The weighting factor was chosen based on goodness-of-fit criteria including coefficient of determination (r2), the back-calculated concentration of individual calibrators, and minimizing intercept value. Precision and accuracy of the method were determined from QC sample results. Within-run precision and accuracy were assessed from the results from a single
day, while between-run precision and accuracy were determined from the results from multiple runs.
No significant peaks interfering with the quantitation of the agents were detected in the chromatograms of blank plasma. Calibration curves for both agents were linear from 5 to 1,000 ng/mL. The r2values were greater than 0.995. The back-calculated concentration of individual calibrators used to determine the calibration curve ranged from 90 to 100% of the true value. The method’s precision (CV%) was less than 10% and within-run accuracy ranged from 92 to 109% for both agents.
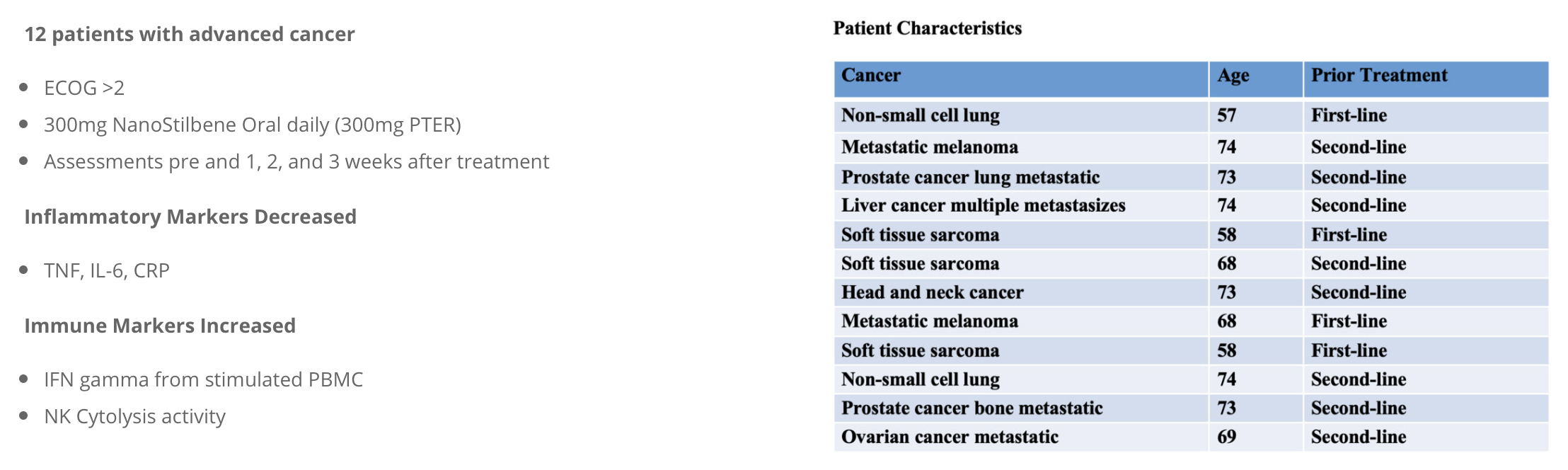
Clinical Trial of NanoStilbene™️ for Immune Derepression in Advanced Cancer
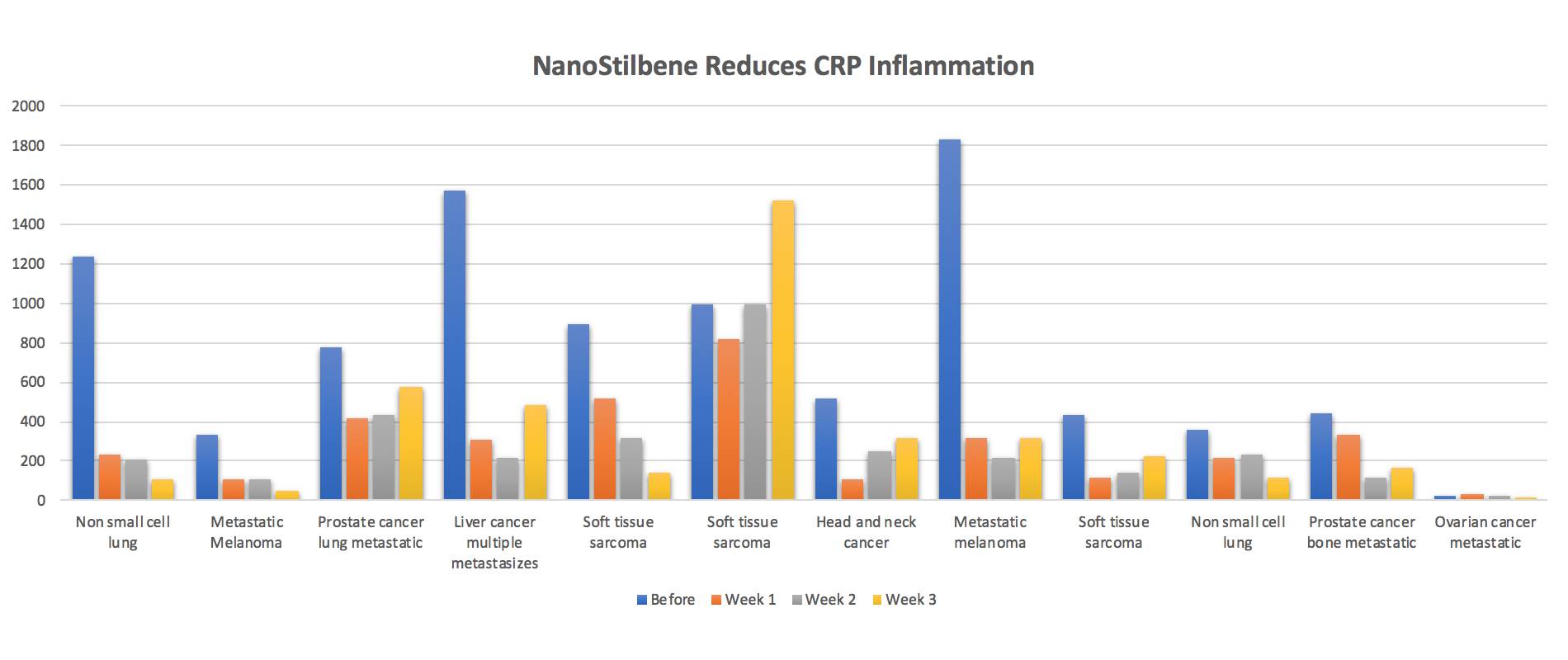
Pterostilbene, being a methyl ether of resveratrol, is known to possess anti-inflammatory and anticancer activity in various model systems. It is known that in advanced cancer, excess inflammatory signaling may be associated with
Given the importance of NK cells in the activity of various Immunotherapeutics, we sought to determine whether administration of a nanoparticle formulation of pterostilbene may reverse cancer associated suppression of NK activity. An initial study in
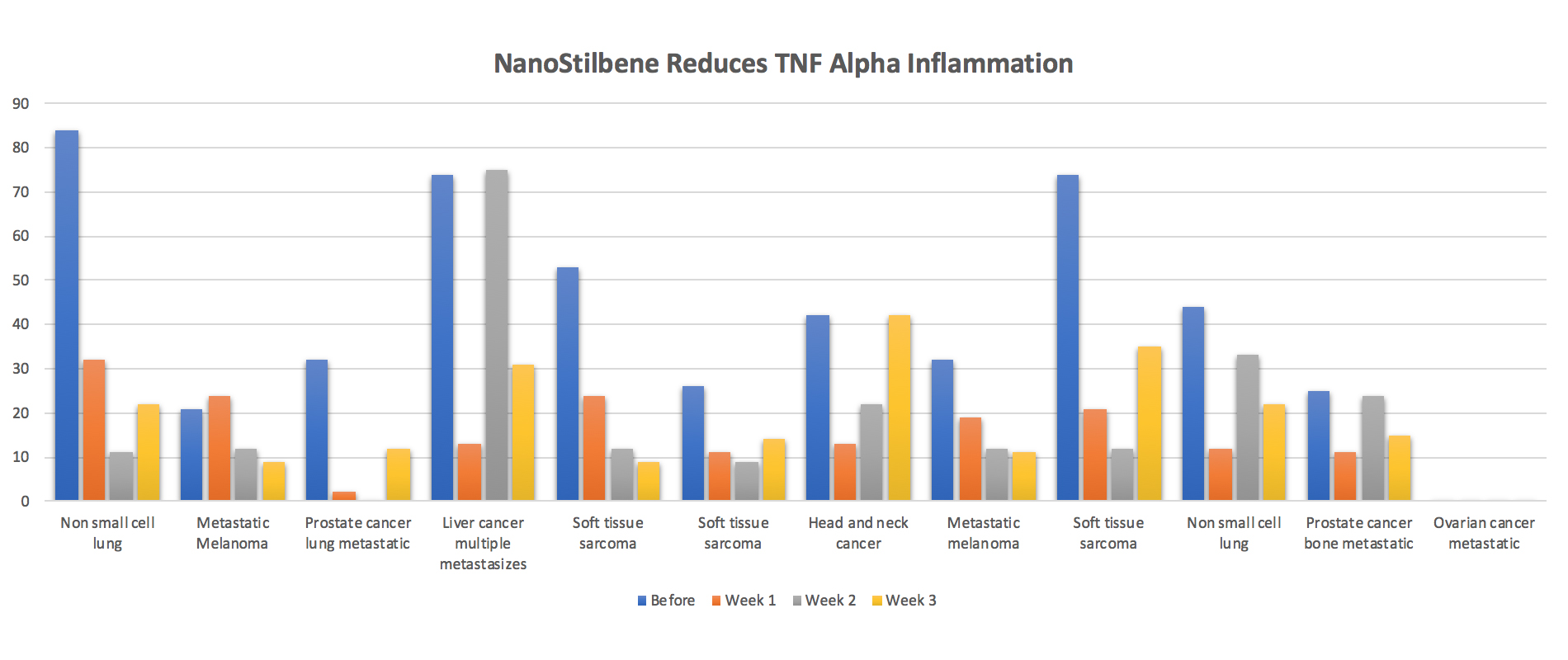
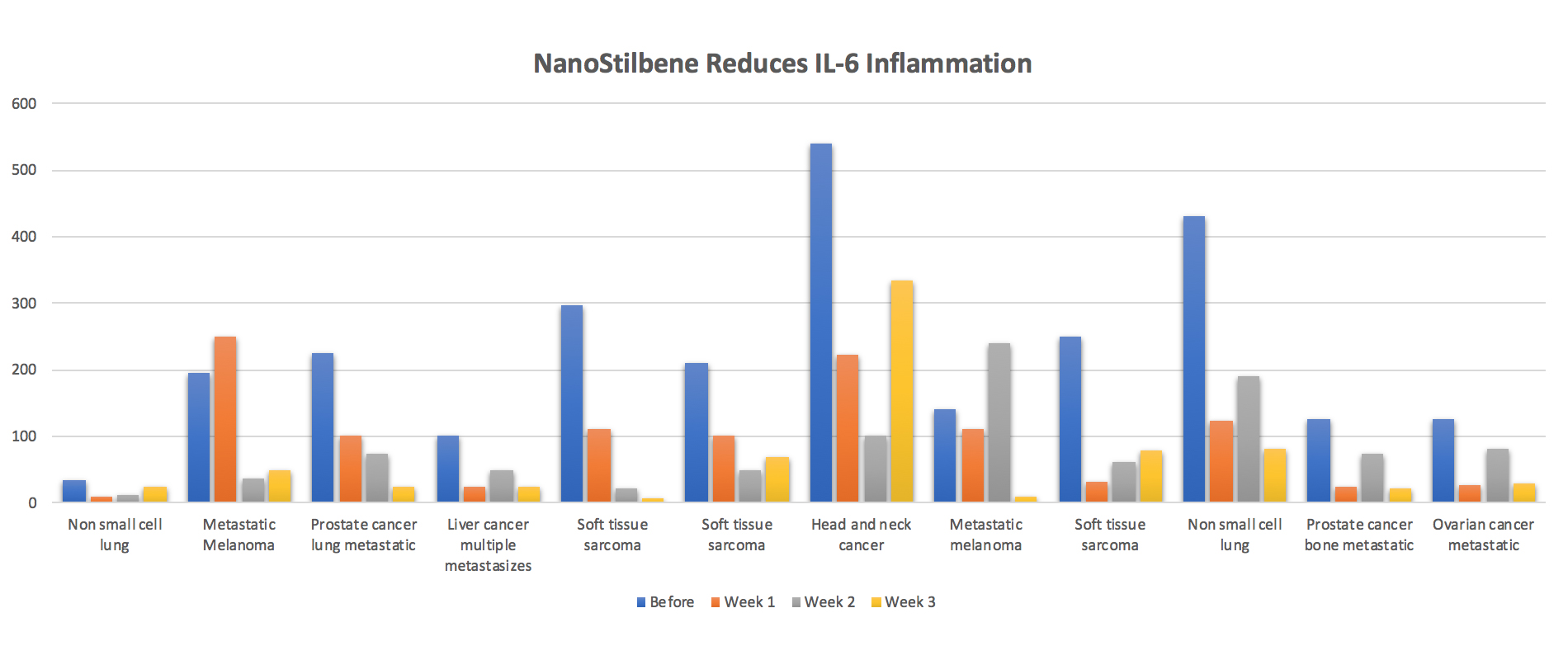
Subsequent to this, the selected NanoStilbene dose was administered to twelve patients with advanced solid cancers for 3 weeks. Daily treatment with 300mg of NanoStilbene caused
TNF-a what is it?
Tumour Necrosis
TNF inhibitors are drugs that help stop inflammation. They’re used to treat diseases like rheumatoid arthritis (RA), juvenile arthritis, psoriatic arthritis, plaque psoriasis, ankylosing spondylitis, ulcerative colitis (UC), and Crohn’s disease. They’re also called TNF blockers, biologic therapies, or anti-TNF drugs.
IL-6 what is it?
IL-6 or Interleukin 6, is an interleukin that acts as both a pro-inflammatory cytokine and an anti-inflammatory myokine. In humans, it is encoded by the IL6 gene. In addition, osteoblasts secrete IL-6 to stimulate osteoclast formation.
Interleukin inhibitors are immunosuppressive agents that inhibit the action of interleukins. Interleukins are a group of cytokines that are synthesized by lymphocytes, monocytes, macrophages, and certain other cells. They function especially in the regulation of the immune system.
CRP what is it?
CRP or C-reactive Protein is an annular, pentameric protein found in blood plasma, whose circulating concentrations rise in response to inflammation. It is an acute-phase protein of hepatic origin that increases following interleukin-6 secretion by macrophages and T cells.
Lowering of CRP may be seen with the use of statin drugs even without significant improvement of the cholesterol profile.
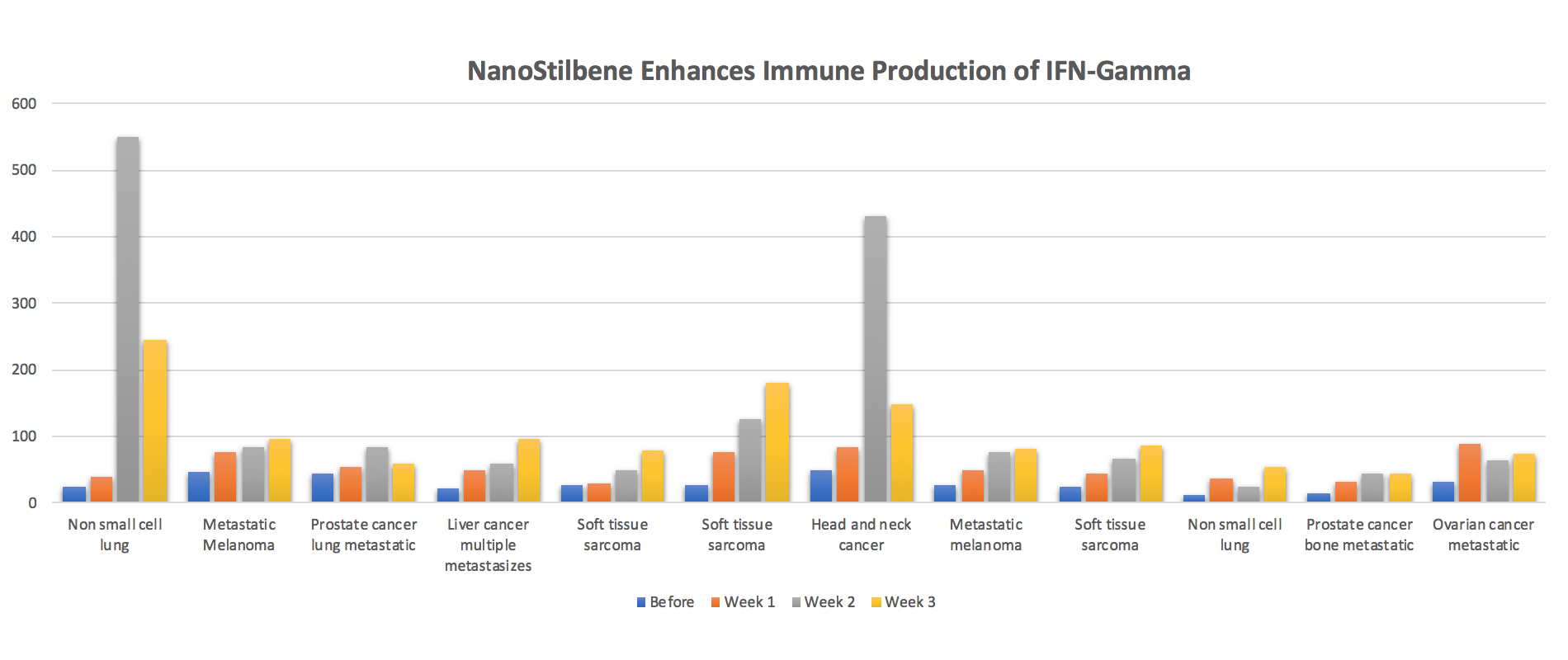
IFN-gamma what is it?
IFN-gamma(IFNγ), or type II interferon, is a cytokine that is critical for innate and adaptive immunity against viral, some bacterial and protozoal infections. IFNγ is an important activator of macrophages and inducer of Class II major histocompatibility complex (MHC) molecule expression.
IFN–gamma has long been recognized as a signature proinflammatory cytokine that plays a central role in inflammation and autoimmune disease. There is now emerging evidence indicating that IFN–gamma possesses unexpected properties as a master regulator of immune responses and inflammation.
NK cell what is it?
Natural killer cells (also known as NK cells, K cells, and killer cells) are a type of lymphocyte (a white blood cell) and a component of the innate immune system. NK cells play a major role in the host-rejection of both tumors and virally infected cells.
NK cells are activated in response to interferons or macrophage-derived cytokines. They serve to contain viral infections while the adaptive immune response generates antigen-specific cytotoxic T cells that can clear the infection. NK cells work to control viral infections by secreting IFNγ and TNFα.
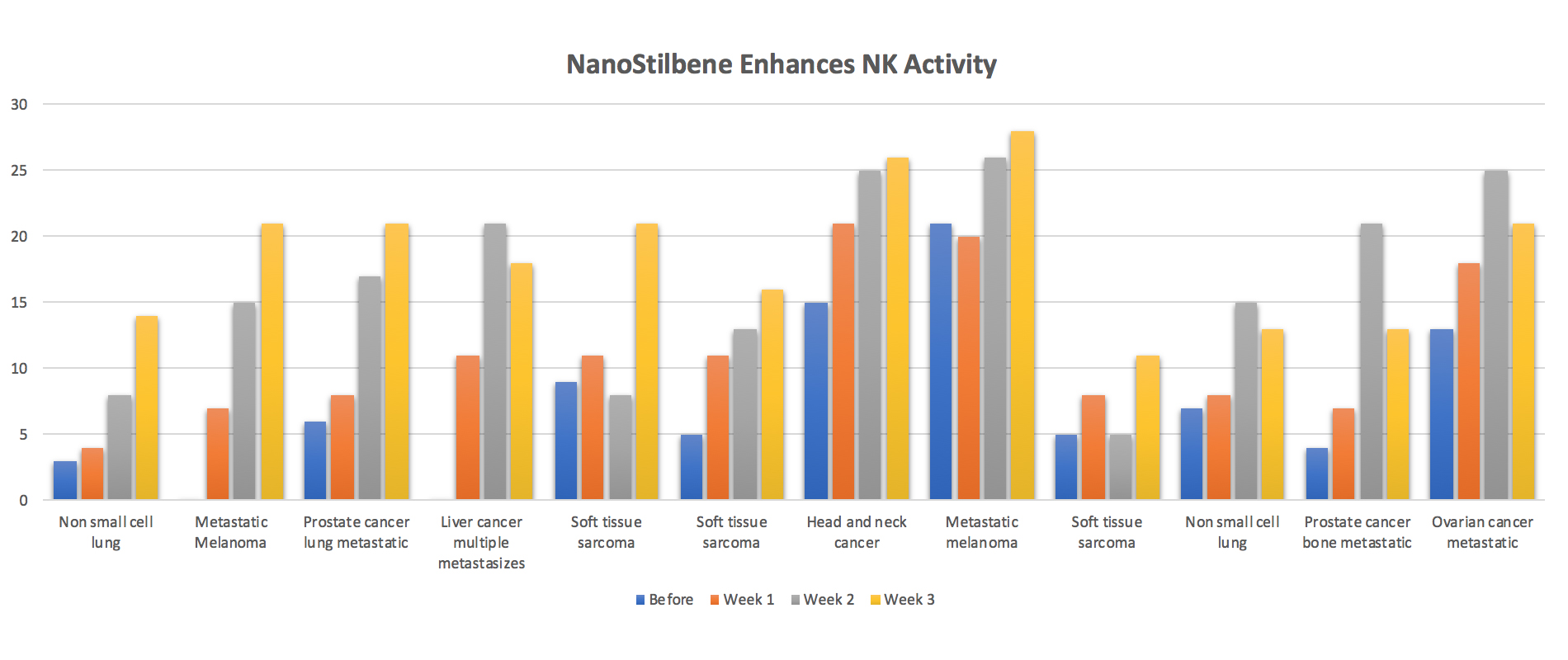
Additionally, NK cytotoxicity was augmented. These results suggest that NanoStilbene may be a useful adjuvant to immunotherapy of cancer rescuing T cell and NK cell activities.
Augmentation of NK cell function may stimulate
*The data provided here is partial and does not contain all materials submitted for publication and is preliminary until peer review is complete. These statements have not been evaluated by the Food and Drug Administration. These products are not intended to diagnose, treat, cure, or prevent any disease.
References:
[1] Montorsi, P., et al., The artery size hypothesis: a macrovascular link between erectile dysfunction and coronary artery disease. Am J Cardiol, 2005. 96(12B): p. 19M-23M.
[2] Hill, J.M., et al., Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med, 2003. 348(7): p. 593-600.
[3] Hughes, A.D., et al., Reduced endothelial progenitor cells in European and South Asian men with atherosclerosis. Eur J Clin Invest, 2007. 37(1): p. 35-41.
[4] Wang, H.Y., et al., [Number of circulating endothelial progenitor cells inversely correlate with the severity of coronary artery disease in patients with stable coronary artery disease]. Zhonghua Xin Xue Guan Bing Za Zhi, 2005. 33(5): p. 425-7.
[5] Fadini, G.P., et al., Number and function of endothelial progenitor cells as a marker of severity for diabetic vasculopathy. Arterioscler Thromb Vasc Biol, 2006. 26(9): p. 2140-6.
[6] Kunz, G.A., et al., Circulating endothelial progenitor cells predict coronary artery disease severity. Am Heart J, 2006. 152(1): p. 190-5.
[7] Foresta, C., et al., Circulating endothelial progenitor cells in subjects with erectile dysfunction. Int J Impot Res, 2005. 17(3): p. 288-90.
[8] Baumhakel, M., et al., Circulating endothelial progenitor cells correlate with erectile function in patients with coronary heart disease. Eur Heart J, 2006. 27(18): p. 2184-8.
[9] Esposito, K., et al., Circulating CD34+ KDR+ endothelial progenitor cells correlate with erectile function and endothelial function in overweight men. J Sex Med, 2009. 6(1): p. 107-14.
[10] Billups, K.L., et al., Relation of C-reactive protein and other cardiovascular risk factors to penile vascular disease in men with erectile dysfunction. Int J Impot Res, 2003. 15(4): p. 231-6.
[11] Giugliano, F., et al., Erectile dysfunction associates with endothelial dysfunction and raised proinflammatory cytokine levels in obese men. J Endocrinol Invest, 2004. 27(7): p. 665-9.
[12] Yasuda, M., et al., Salivary 8-OHdG: a useful biomarker for predicting severe ED and hypogonadism. J Sex Med, 2008. 5(6): p. 1482-91.
[13] Azadzoi, K.M., et al., Oxidative stress and neurodegeneration in penile ischaemia. BJU Int. 105(3): p. 404-10.
[14] Vlachopoulos, C., et al., Unfavourable endothelial and inflammatory state in erectile dysfunction patients with or without coronary artery disease. Eur Heart J, 2006. 27(22): p. 2640-8.
[15] Carneiro, F.S., et al., TNF-alpha knockout mice have increased corpora cavernosa relaxation. J Sex Med, 2009. 6(1): p. 115-25.
[16] Carneiro, F.S., et al., TNF-alpha infusion impairs corpora cavernosa reactivity. J Sex Med, 2009. 6 Suppl 3: p. 311-9.
[17] Oh, J.S., et al., The effect of anti-tumor necrosis factor agents on sexual dysfunction in male patients with ankylosing spondylitis: a pilot study. Int J Impot Res, 2009. 21(6): p. 372-5.
[18] Grisar, J., et al., Endothelial progenitor cells in active rheumatoid arthritis: effects of tumour necrosis factor and glucocorticoid therapy. Ann Rheum Dis, 2007. 66(10): p. 1284-8.
[19] Dou, Q.P., Molecular mechanisms of green tea polyphenols. Nutr Cancer, 2009. 61(6): p. 827-35.
[20] im, W., et al., Effect of green tea consumption on endothelial function and circulating endothelial progenitor cells in chronic smokers. Circ J, 2006. 70(8): p. 1052-7.
[21] Kondoh, N., et al., Salvage therapy trial for erectile dysfunction using phosphodiesterase type 5 inhibitors and vitamin E: preliminary report. Aging Male, 2008. 11(4): p. 167-70.
[22] Shukla, N., et al., The administration of folic acid improves erectile function and reduces intracavernosal oxidative stress in the diabetic rabbit. BJU Int, 2009. 103(1): p. 98-103.
[23] Ryu, J.K., et al., Free radical-scavenging activity of Korean red ginseng for erectile dysfunction in non-insulin-dependent diabetes mellitus rats. Urology, 2005. 65(3): p. 611-5.
[24] Morano, S., et al., Antioxidant treatment associated with sildenafil reduces monocyte activation and markers of endothelial damage in patients with diabetic erectile dysfunction: a double-blind, placebo-controlled study. Eur Urol, 2007. 52(6): p. 1768-74.
[25] Tateishi-Yuyama, E., et al., Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: a pilot study and a randomised controlled trial. Lancet, 2002. 360(9331): p. 427-35.
[26] Subramaniyam, V., et al., Bone marrow mobilization with granulocyte macrophage colony-stimulating factor improves endothelial dysfunction and exercise capacity in patients with peripheral arterial disease. Am Heart J, 2009. 158(1): p. 53-60 e1.
[27] Watanabe, T., et al., Postischemic intraventricular administration of FGF-2 expressing adenoviral vectors improves neurologic outcome and reduces infarct volume after transient focal cerebral ischemia in rats. J Cereb Blood Flow Metab, 2004. 24(11): p. 1205-13.
[28] Aviles, R.J., B.H. Annex, and R.J. Lederman, Testing clinical therapeutic angiogenesis using basic fibroblast growth factor (FGF-2). Br J Pharmacol, 2003. 140(4): p. 637-46.
[29] Jeon, O., et al., Synergistic effect of sustained delivery of basic fibroblast growth factor and bone marrow mononuclear cell transplantation on angiogenesis in mouse ischemic limbs. Biomaterials, 2006. 27(8): p. 1617-25.
[30] Xie, D., et al., Intracavernosal basic fibroblast growth factor improves vasoreactivity in the hypercholesterolemic rabbit. J Sex Med, 2006. 3(2): p. 223-32.
[31] Suetomi, T., et al., Effect of basic fibroblast growth factor incorporating gelatin microspheres on erectile function in the diabetic rat. J Urol, 2005. 173(4): p. 1423-8.
[32] Dai, Q., et al., Systemic basic fibroblast growth factor induces favorable histological changes in the corpus cavernosum of hypercholesterolemic rabbits. J Urol, 2003. 170(2 Pt 1): p. 664-8.
[33] Foresta, C., et al., Reduced number of circulating endothelial progenitor cells in hypogonadal men. J Clin Endocrinol Metab, 2006. 91(11): p. 4599-602.
[34] Lamina, S., C.G. Okoye, and T.T. Dagogo, Therapeutic effect of an interval exercise training program in the management of erectile dysfunction in hypertensive patients. J Clin Hypertens (Greenwich), 2009. 11(3): p. 125-9.
[35] Sighinolfi, M.C., et al., Immediate improvement in penile hemodynamics after cessation of smoking: previous results. Urology, 2007. 69(1): p. 163-5.
[36] Mobius-Winkler, S., et al., Time-dependent mobilization of circulating progenitor cells during strenuous exercise in healthy individuals. J Appl Physiol, 2009. 107(6): p. 1943-50.
[37] Luk, T.H., et al., Habitual physical activity is associated with endothelial function and endothelial progenitor cells in patients with stable coronary artery disease. Eur J Cardiovasc Prev Rehabil, 2009. 16(4): p. 464-71.
[38] Kondo, T., et al., Smoking cessation rapidly increases circulating progenitor cells in peripheral blood in chronic smokers. Arterioscler Thromb Vasc Biol, 2004. 24(8): p. 1442-7.
[39] Peter B, Bosze S, Horvath R. Biophysical characteristics of proteins and living cells exposed to the green tea polyphenol epigallocatechin-3-gallate (EGCg): review of recent advances from molecular mechanisms to nanomedicine and clinical trials. Eur Biophys J. 2017;46(1):1–24.
[40] Tipoe GL, Leung TM, Hung MW, Fung ML. Green tea polyphenols as an anti-oxidant and anti-inflammatory agent for cardiovascular protection. Cardiovasc Hematol Disord Drug Targets. 2007;7:135-144.
[41] Tang N, Wu Y, Zhou B, Wang B, Yu R. Green tea, black tea consumption and risk of lung cancer: a meta-analysis. Lung Cancer. 2009;65:274-283.
[42] Seely D, Mills EJ, Wu P, Verma S, Guyatt GH. The effects of green tea consumption on incidence of breast cancer and recurrence of breast cancer: a systematic review and meta-analysis. Integr Cancer Ther. 2005;4:144-155.
[43] Clement Y. Can green tea do that? A literature review of the clinical evidence. Prev Med. 2009;49:83-87.
[44] Liang W, Lee AH, Binns CW. Tea drinking, diet and ischemic stroke prevention in China: a future perspective. Expert Rev Cardiovasc Ther. 2009;7:1447-1454.
[45] Hodgson JM. Effects of tea and tea flavonoids on endothelial function and blood pressure: a brief review. Clin Exp Pharmacol Physiol. 2006;33:838-841.
[46] Kim W, Jeong MH, Cho SH, Yun JH, Chae HJ, Ahn YK, Lee MC, Cheng X, Kondo T, Murohara T. Effect of green tea consumption on endothelial function and circulating endothelial progenitor cells in chronic smokers. Circ J. 2006;70:1052-1057.
[47] Oyama J, Maeda T, Sasaki M, Kozuma K, Ochiai R, Tokimitsu I, Taguchi S, Higuchi Y, Makino N. Green tea catechins improve human forearm vascular function and have potent anti-inflammatory and anti-apoptotic effects in smokers. Intern Med. 2010;49:2553-2559.
[48] Duffy SJ, Keaney JF, Holbrook M, Gokce N, Swerdloff PL, Frei B, Vita JA. Short- and long-term black tea consumption reverses endothelial dysfunction in patients with coronary artery disease. Circulation. 2001;104:151-156.
[49] Grassi D, Aggio A, Onori L, Croce G, Tiberti S, Ferri C, Ferri L, Desideri G. Tea, flavonoids, and nitric oxide-mediated vascular reactivity. J Nutr. 2008;138:1554S-1560S.
[50] Loke WM, Hodgson JM, Proudfoot JM, McKinley AJ, Puddey IB, Croft KD. Pure dietary flavonoids quercetin and (-)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. Am J Clin Nutr. 2008;88:1018-1025.
[51] Persson IA, Josefsson M, Persson K, Andersson RG. Tea flavanols inhibit angiotensin-converting enzyme activity and increase nitric oxide production in human endothelial cells. J Pharm Pharmacol. 2006;58:1139-1144.
[52] Mills TM, Chitaley K, Lewis RW. Vasoconstrictors in erectile physiology. Int J Impot Res. 2001;13 Suppl 5:S29-S34.
[53] Jackson G. Sexual response in cardiovascular disease. J Sex Res. 2009;46:233-236.